Outcomes of Orbital Atherectomy in Patients With Critical Limb Threatening Ischemia and Diabetes
Momodou L. Jammeh, MD1; Julia Suggs, MD1; George L. Adams, MD, MHS2; Ehrin J. Armstrong, MD3; Jihad A. Mustapha, MD4; Mohamed A. Zayed, MD, PhD1,5,6,7
ISSN: 2694-3026
J CRIT LIMB ISCHEM 2022;2(2):E29-E37. Epub 2022 April 12.
Abstract
Purpose. Patients with diabetes and critical limb threatening ischemia (CLTI) are at significantly higher risk of limb loss and death. We evaluate the outcomes of orbital atherectomy (OA) for the treatment of CLTI in patients with and without diabetes. Methods. A retrospective analysis of the LIBERTY 360 study was performed to evaluate baseline demographics and periprocedural outcomes between patients with CLTI, and with and without diabetes. Hazard ratios (HRs) were determined with Cox regression to examine the impact of OA in patients with diabetes and CLTI over a 3-year follow-up. Results. A total of 289 patients (201 with diabetes, 88 without diabetes) with Rutherford classification 4-6 were included. Patients with diabetes had a higher proportion of renal disease (48.3% vs 28.4%; P<.01), prior minor/major limb amputation (26% vs 8%; P<.01), and presence of wounds (63.2% vs 48.9%; P=.03). Operative times, radiation dosages, and contrast volumes were similar between groups. The rate of distal embolization was higher in patients with diabetes (7.8% vs 1.9%; P=.01; odds ratio, 4.33; 95% confidence interval, 0.99-18.88; P=.05). However, at 3 years post procedure, patients with diabetes had no differences in freedom from target-vessel/target-lesion revascularization (HR, 1.09; P=.73), major adverse events (HR, 1.25; P=.36), major target-limb amputation (HR, 1.74; P=.39), and death (HR, 1.11; P=.72). Conclusion. The LIBERTY 360 study observed high limb preservation and low major adverse events in patients with diabetes and CLTI. Higher distal embolization was observed with OA in patients with diabetes, but the odds ratio did not indicate a significant difference in risk between groups.
J CRIT LIMB ISCHEM 2022;2(2):E29-E37. Epub 2022 April 12.
Key words: amputation, critical limb threatening ischemia, diabetes, endovascular revascularization, orbital atherectomy
Introduction
Peripheral artery disease (PAD) impacts an estimated 8-12 million people, with a relative increase in prevalence to 24% between 2000 and 2010 in the United States.1-3 Among patients with symptomatic progression of the disease, only one-third will adhere to risk-factor modification in the form of appropriate diabetes glycemic control, dietary changes, and functional exercise programs.4-7 Additionally, it is estimated that nearly 50% of individuals with critical limb threatening ischemia (CLTI; rest pain or with evidence of lower-extremity/foot tissue loss) will progress to limb loss within 2 years.8 Therefore, prompt revascularization is often necessary for symptom resolution and limb salvage in patients with CLTI,9-11 particularly in individuals with diabetes, who are traditionally known to be more prone to CLTI-related complications.12-15 It is widely accepted that individuals with diabetes and CLTI are at higher risk of limb loss if urgent revascularization is not performed successfully.
Diabetes is a chronic metabolic condition characterized by abnormal glycemic control, and is one of the strongest risk factors for progression of PAD.2,12 Individuals with diabetes who progress to CLTI have a 30%-45% risk of lower-extremity amputation, and an estimated 1-year mortality rate of 20% following amputation.16-18 Historical data also suggest that patients with diabetes and CLTI are more likely to suffer from poor outcomes following endovascular revascularization procedures.18 However, more recent studies advocate that earlier revascularization with catheter-based interventions may improve limb-salvage rates and reduce major adverse events (MAEs), particularly in vulnerable populations with diabetes and CLTI.19,20 The recent global guidelines for the management of CLTI support an aggressive approach to revascularization of patients with CLTI, but indicate that there is continued debate regarding the clinical efficacy of modern endovascular techniques.21
Orbital atherectomy (OA) technology utilizes rotational techniques to circumferentially debulk and modify the luminal wall calcium as a means to create a flow lumen channel through obstructed peripheral arterial segments.22,23 While it is suggested that patients with diabetes and CLTI may benefit from OA due to a higher incidence of medial calcific disease in smaller below-the-knee tibial arteries, there is currently limited clinical evidence that supports this premise. The LIBERTY 360 study captured detailed clinical characteristics of patients with symptomatic PAD undergoing endovascular revascularization and compiled both clinical as well as procedural outcomes.24,25 To elucidate the impact of OA on patients with diabetes and CLTI, we conducted a subgroup analysis of the LIBERTY 360 study and evaluated patient demographics, clinical and procedural data, and lower-extremity outcomes over a 3-year follow-up period.
Methods
Study design. The LIBERTY 360 study is a prospective, observational, multicenter, clinical study examining the predictors of clinical outcomes in patients undergoing endovascular treatment of lesions in the distal superficial femoral, popliteal, tibial peroneal trunk, anterior, posterior, or peroneal tibial arteries. The study rationale, design, and overall analysis have been previously reported.25 The study protocol was developed by a steering committee, including principal investigators, representatives from the study core laboratories, and the sponsor (Cardiovascular Systems, Inc); the sponsor was responsible for the oversight of the study. The protocol was ultimately approved by the institutional review board at each participating institution and registered on ClinicalTrials.gov (NCT01855412).
Study population. The LIBERTY 360 study enrolled patients >18 years old with symptomatic PAD (Rutherford classification [RC] 2 to 6) and undergoing peripheral revascularization for lesion(s) located 10 cm above the medial epicondyle of the femur (mid-superficial femoral artery) to the digital arteries. Patients that required conversion from endovascular to surgical revascularization were excluded from the study. Detailed patient inclusion and exclusion criteria to the LIBERTY 360 study have been previously described.23-25 Our subgroup analysis included only patients with CLTI defined as RC 4, 5, or 6 who underwent OA (all lesions treated with Diamondback/Stealth; Cardiovascular Systems, Inc) and stratified into groups with diabetes and without diabetes.
Study outcomes. Multiple prespecified outcomes were collected in the LIBERTY 360 study and assessed at various postprocedure time points. The primary outcomes of this analysis consisted of lesion-level success and death or major amputation within 30 days. Lesion success was defined as <50% residual stenosis for each lesion treated during the index procedure without severe angiographic complications (flow-limiting dissections [type C-F], perforation, abrupt closure, or distal embolization). Perioperative outcomes reported include length of stay, discharge location, and access-site complications. MAEs were defined as death within 30 days of the index procedure, unplanned major amputation of the target limb, and target-vessel revascularization as assessed by the angiographic core laboratory (SynvaCor/Prairie Educational and Research Cooperative) when angiographic images were available. A wound was defined as healed at the follow-up visit when the area was reduced to zero, including cases where amputation was performed and the surgical site was completely healed.
Statistical analysis. Numeric data are presented as mean ± standard deviation; P-values were generated using analysis of variance (ANOVA) for continuous variables and Kruskal-Wallis test for discrete continuous variables. Categorical data are presented as number (%) and P-values comparing patients with diabetes and those without diabetes were generated using a Monte Carlo Approximation of the Fisher’s exact test. Imputation of severe angiographic complications for lesion success of core-lab identified lesions was performed by using site data when the core lab was unable to perform angiographic assessment; unadjusted odds ratios were calculated using a logistic regression model. The Kaplan-Meier time-to-event methodology was used to estimate event rates, the log-rank test was used to compare rates over time, and a Cox proportional hazard model was used to create hazard ratios. Statistical analyses were conducted by NAMSA using SAS Software System (SAS Institute, Inc) with statistical significance set at P<.05.
Results
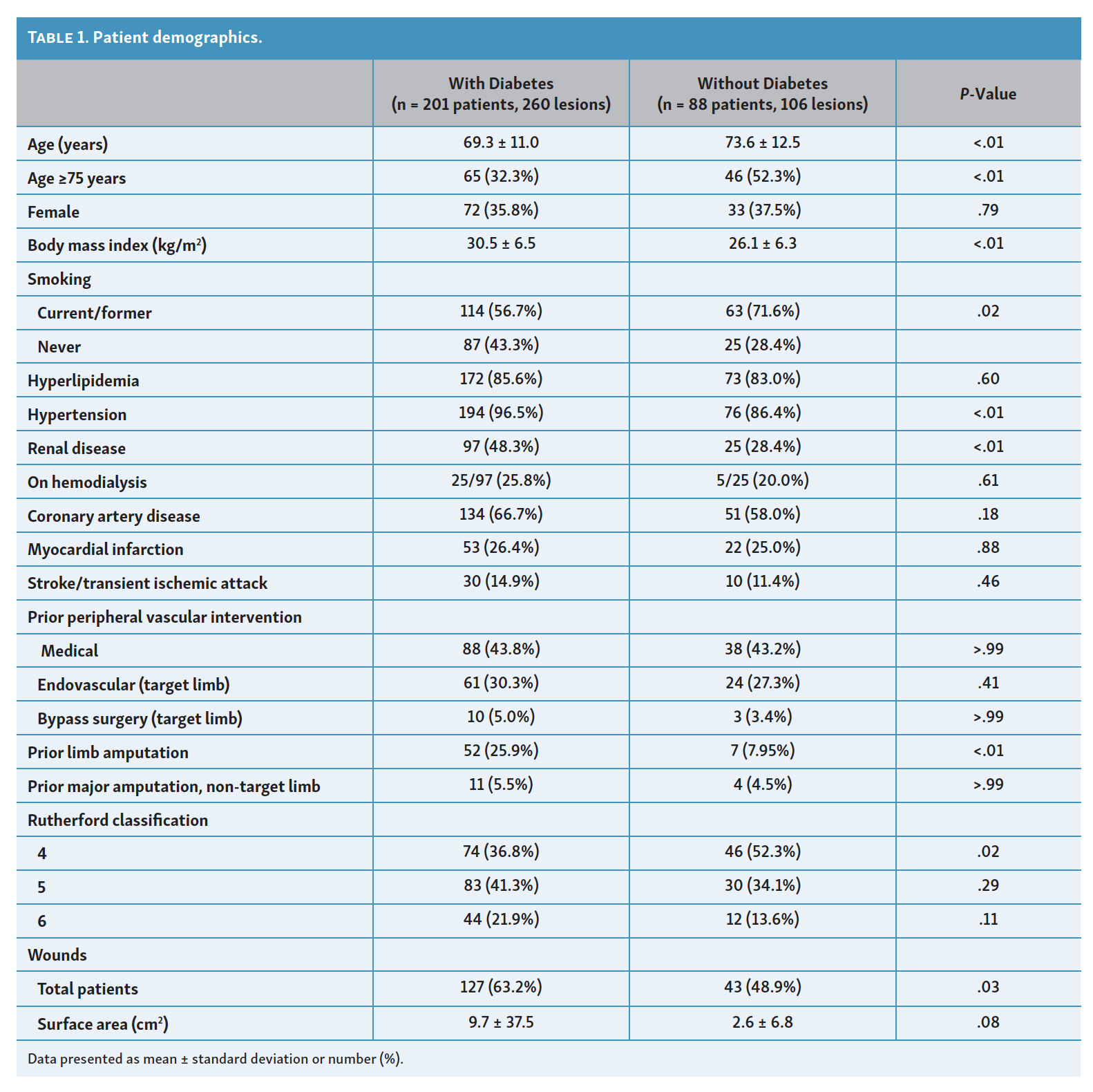
Patient characteristics. Of the 1204 subjects enrolled in the LIBERTY 360 study from May 2013 to February 2016, a total of 289 patients had CLTI (120 RC 4, 113 RC 5, and 56 RC 6). Patient characteristics, lesion data, and procedural details are summarized in Table 1, Table 2, and Table 3, respectively. Among patients with CLTI, there were 201 patients with diabetes and 88 patients without diabetes. Follow-up was available for 89% vs 85% of patients with and without diabetes at 30 days, and 42% vs 40% at 3 years.
{kind=link}
{kind=link}
{kind=link}



As summarized in Table 1, patients with diabetes and CLTI tended to be younger (69.3 ± 11.0 years vs 73.6 ± 12.5 years; P<.01), comprised a smaller percentage of patients over the age of 75 years (32.3% vs 52.3%; P<.01), and more frequently had renal disease (48.3% vs 28.4%; P<.01), hypertension (96.5% vs 86.4%; P<.01), and a higher body mass index (30.5 ± 6.5 kg/m2 vs 26.1 ± 6.3 kg/m2; P<.01). Patients with diabetes were also more likely to have never smoked (43.3% vs 28.4%; P=.02) and had similar rates of myocardial infarction (26.4% vs 25.0%; P=.88) and stroke/transient ischemic attack (14.9% vs 11.4%; P=.46). There was no difference in prior target-limb peripheral vascular interventions between patients with and without diabetes. Previous minor/major limb amputations were more likely in the diabetes cohort (26% vs 8%; P<.01), with all prior target-limb amputations limited to toes or foot and no above-ankle amputations. In addition, patients with diabetes and CLTI were more likely to have unhealed wounds at the time of intervention (63.2% vs 48.9%; P=.03) and those without diabetes predominantly had RC 4 CLTI (36.8% vs 52.3%; P=.02).
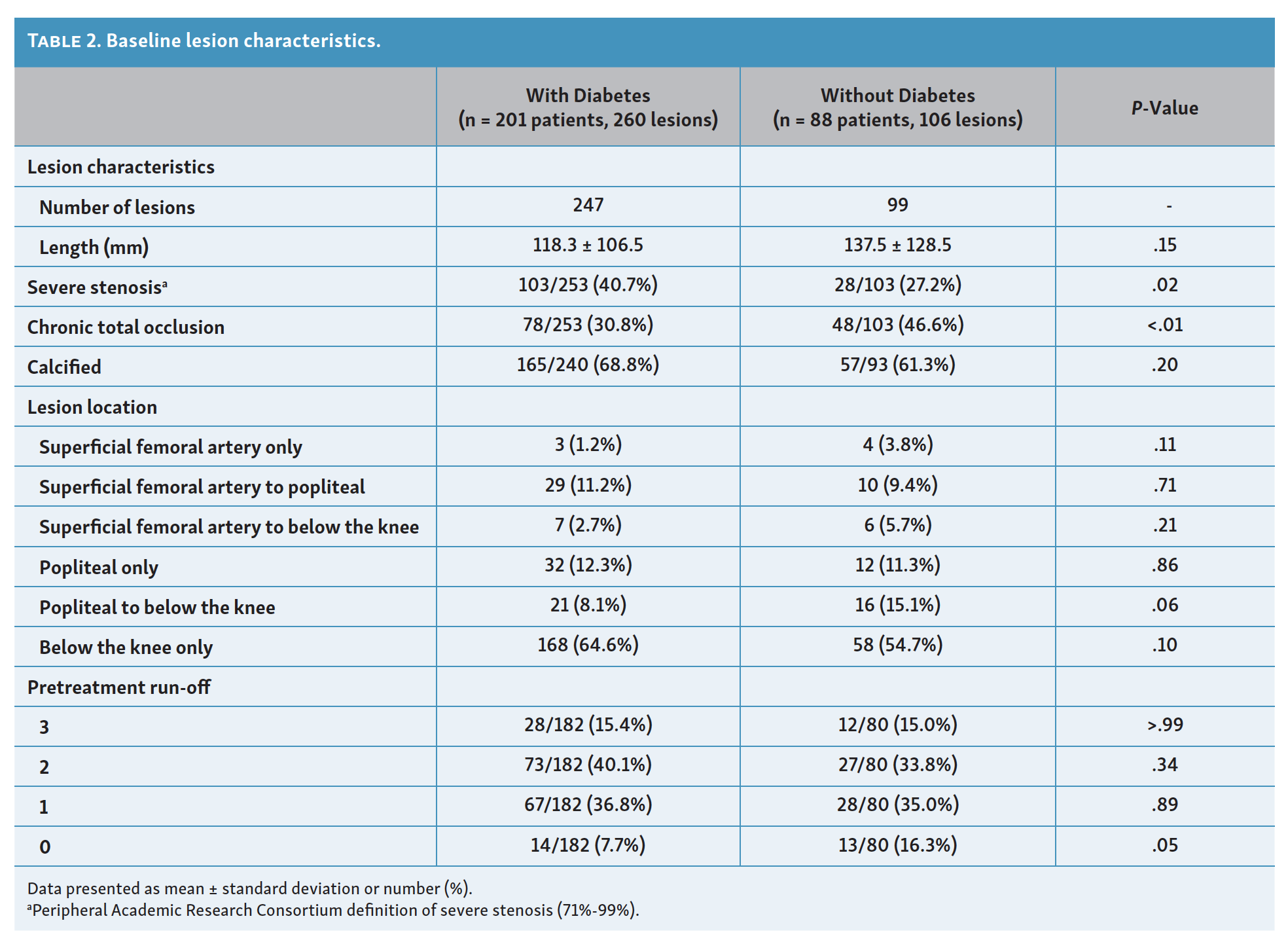
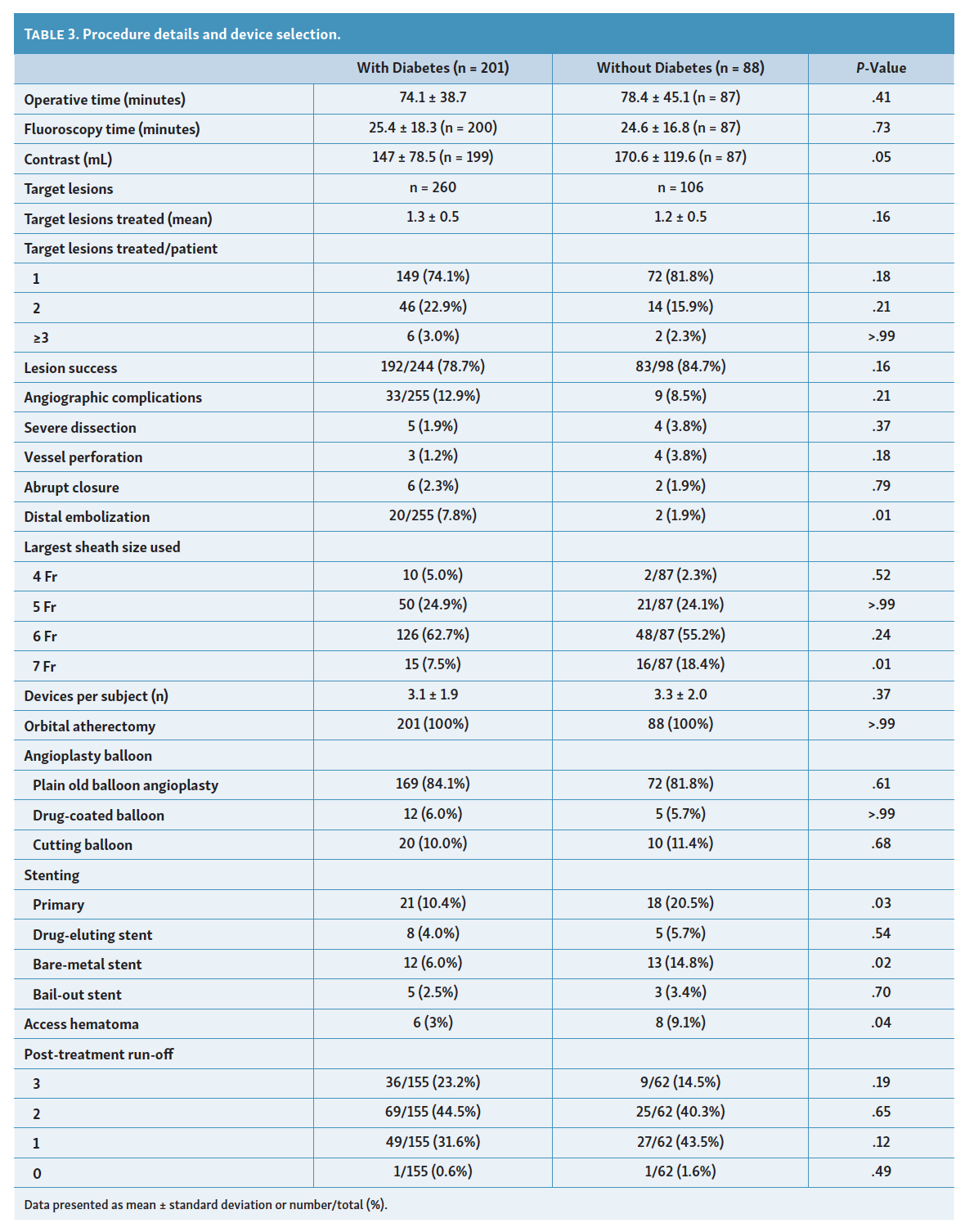
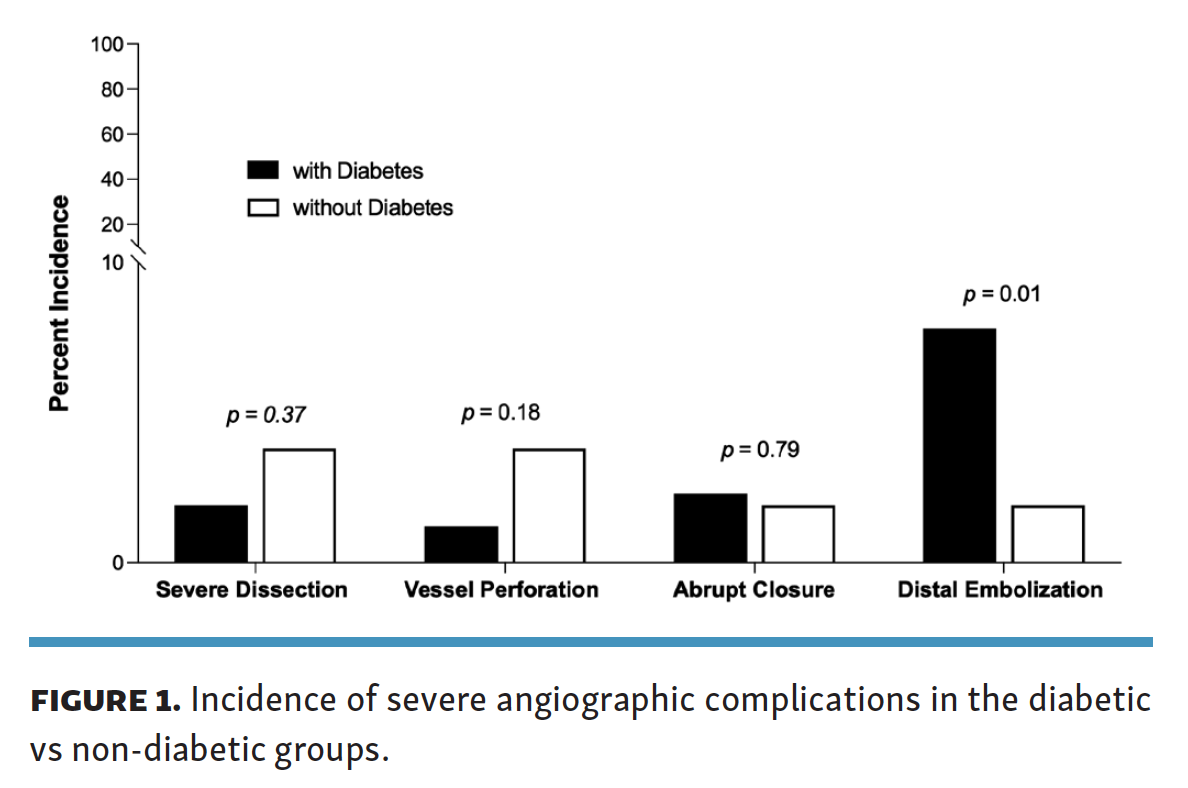
Lesion and procedure outcomes. A total of 260 lesions (1.3 ± 0.5 lesions per patient) were treated in patients with diabetes and CLTI and 106 lesions were treated in those without diabetes (1.2 ± 0.5 lesions per patient) (Table 2). Compared with patients with no CLTI,24 patients with CLTI that we evaluated in our subgroup analysis overall had more severe lesion characteristics (Table 2). However, we observed no significant difference in the rates of infrapopliteal disease (64.6% vs 54.7%; P=.10), average lesion length (118.3 ± 106.5 mm vs 137.5 ± 128.5 mm; P=.15), or the prevalence of calcified lesions (68.8% vs 61.3%; P=.20) between patients with CLTI and with vs without diabetes. While severe stenosis (71%-99%) was more common in patients with diabetes (40.7% vs 27.2%; P=.02), those with diabetes were less likely to have chronic total occlusions (30.8% vs 46.6%; P<.01) and had a lower incidence of zero run-off vessels (7.7% vs 16.3%; P=.05). The use of balloon angioplasty was similar between patients with vs without diabetes, ie, plain old balloon angioplasty (84.1% vs 81.8%; P=.61), drug-coated balloon (6% vs 5.7%; P>.99), and cutting balloon (10% vs 11.4%; P=.68) (Table 3). Meanwhile, primary stenting (non-bailout preplanned stenting) was less frequent in patients with diabetes (10.4% vs 20.5%; P=.03). Lesion treatment success rate was the same between groups, with similarly low rates of severe dissection or perforation and low rates of bail-out stenting observed across groups (2.5% vs 3.4%; P=.70). Of note, the distal embolization rate was higher in treated lesions of diabetic patients (7.8% vs 1.9%; P=.01; odds ratio [OR], 4.33; 95% confidence interval [CI], 0.99-18.88; P=.05) (Figure 1).
{kind=link}

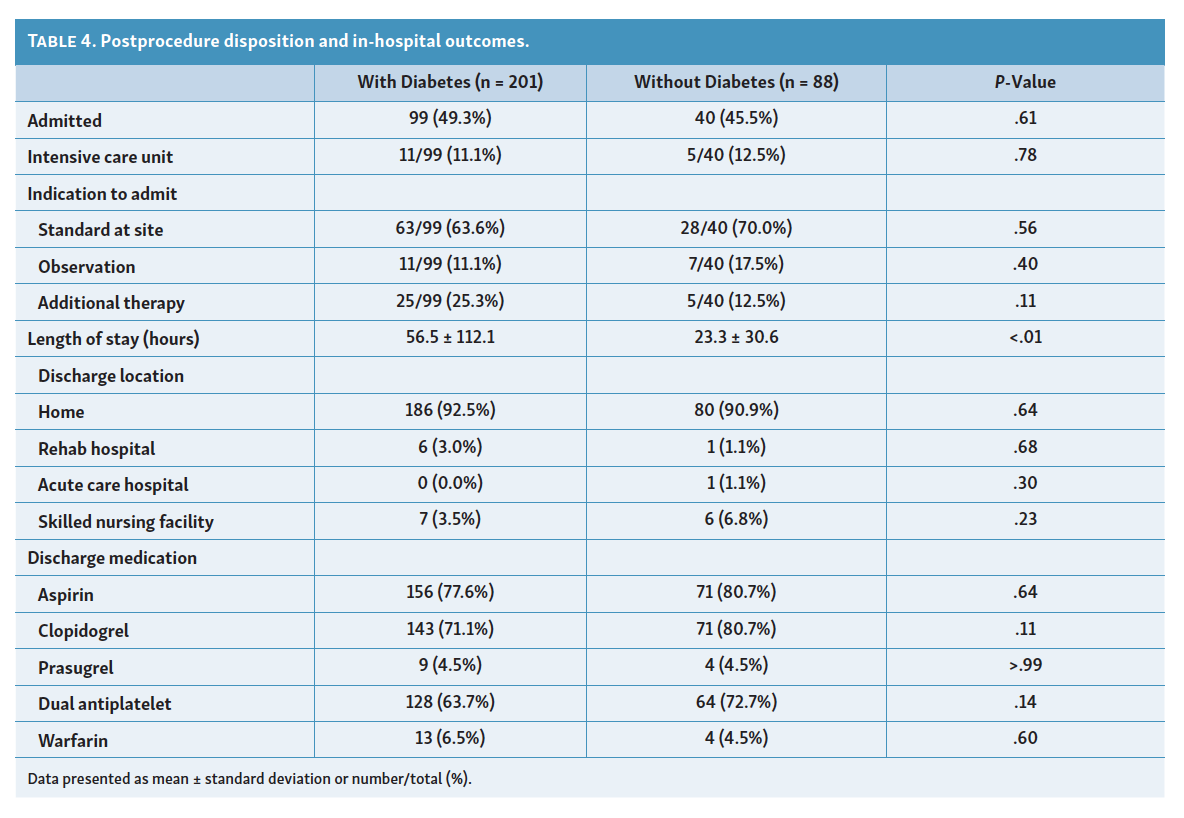
In addition, there was no difference in procedure and total fluoroscopy times between groups, but lower volume of contrast was used in patients with diabetes (147.0 ± 78.5 mL vs 170.6 ± 119.6 mL; P=.05). While in-hospital admission rate, time in intensive care, and discharge location were the same across both groups, patients with diabetes had a longer length of stay (56.5 ± 112.1 hours vs 23.2 ± 30.6 hours; P<.01) (Table 4).
{kind=link}

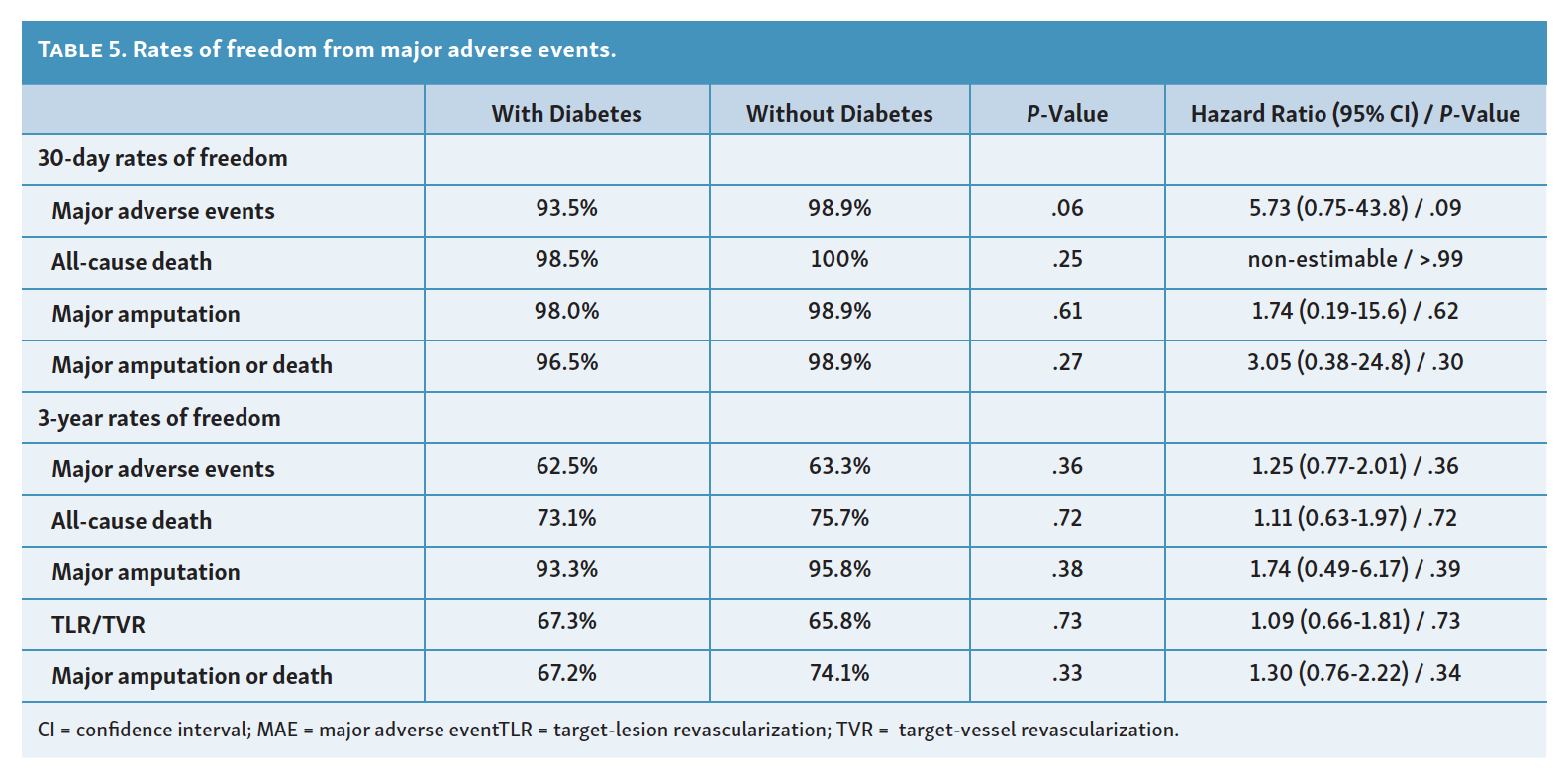
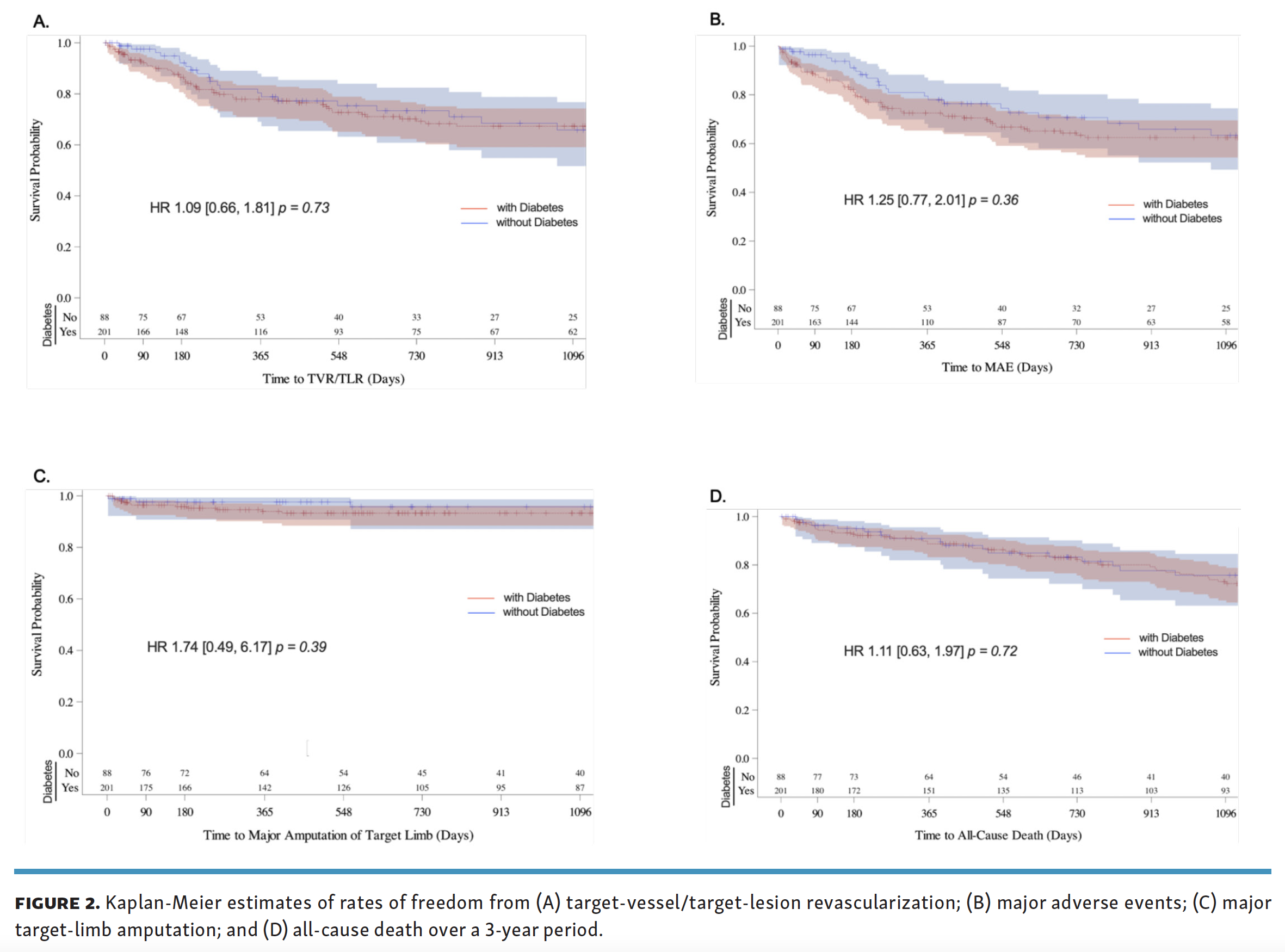
Event rates and wound healing. There was no significant difference in primary outcomes of rates of freedom from all-cause death (hazard ratio [HR], 5.73; 95% CI, 0.75-43.8; P=.09), major target-limb amputation (HR, 1.74; 95% CI, 0.19-15.6; P=.62), and major amputation or death (HR, 3.05; 95% CI, 0.38-24.8; P=.30) within 30 days in patients with diabetes (Table 5). At 3 years, patients with diabetes also had similar rates of freedom from MAEs (62.5% vs 63.3%; HR, 1.25; 95% CI, 0.77-2.01; P=.36), all-cause death (73.1% vs 75.7%; HR, 1.11; 95% CI, 0.63-1.97; P=.72), major target-limb amputation (93.3% vs 95.8%; HR, 1.74; 95% CI, 0.49-6.17; P=.39) and target-lesion/target-vessel revascularization (67.3% vs 65.8%; HR, 1.09; 95% CI, 0.66-1.81; P=.73) (Figure 2). At 12 months, wounds identified at baseline on the target limb had completely healed in 67/88 patients with diabetes (76.1%) and 21/27 patients without diabetes (77.8%). These wound-healing rates increased to 76/78 patients with diabetes (97.4%) and 24/24 patients without diabetes (100%) at 2 years.
{kind=link}
{kind=link}


Discussion
This retrospective subgroup analysis of prospectively collected data from the observational, multicenter LIBERTY 360 trial summarizes the outcomes of OA in 289 patients with CLTI stratified according to diabetes status. Although our study is inherently limited by its retrospective nature, our analysis provides various important observations. First, predisposing risk factors for PAD appeared to be different across patients with or without diabetes. While obesity and chronic kidney disease rates were significantly higher in patients with diabetes, smoking and older age were more common in patients without diabetes. Second, this study demonstrated that patients with CLTI and diabetes benefited from OA to the same extent as patients with no diabetes, which resulted in high rates of limb salvage (>93%) and low rates of MAEs and TLR/TVR over a 3-year period. Additionally, the 3-year mortality rates of 26.9% and 24.3% for patients with and without diabetes were also well below the previously reported 3-year mortality of 40%-60% in patients with CLTI.26,27 It is important to note that we observed high rates of wound healing in both patients with and without diabetes, which may be due to enhanced continued careful outpatient surveillance and follow-up during the prospective study period.
Based on historical data, patients with diabetes carry a significantly higher burden of advanced CLTI with largely infrapopliteal disease, while smokers have more commonly associated occlusive disease in more proximal aortoiliac and femoral-popliteal arterial segments.13,14 Interestingly, in this study, the distribution of infrapopliteal disease was only slightly higher in patients with diabetes, and not significantly different from patients without diabetes (Table 1). Similarly, the severity of vessel-wall calcification and lesion extent were comparable between patients with and without diabetes. This observation may be due to an older cohort of patients without diabetes, who were thus more likely to have a higher peripheral arterial calcific plaque burden. Arterial wall calcification is known to increase with age and in this study, 52% of patients without diabetes relative to 32% of patients with diabetes were >75 years old (Table 1).
Nearly 70% of patients with CLTI treated with OA also had diabetes, the majority of whom had RC 5 or 6 disease. While the rates of wound healing in the current study remained high in both populations, a prolonged period of careful surveillance and follow-up was needed during the course of the study to ensure appropriate data collection. This likely improved podiatric and wound care during the postoperative surveillance period and may have contributed to the impressively high limb-salvage rates. It is also important to note that prior amputations were 3 times more likely in patients with diabetes and overall mortality was also numerically higher in patient with diabetes (Table 1). Overall, these data demonstrate that although patients with diabetes were more vulnerable and at higher risk of limb loss, the incidence of MAEs remained low and comparable to patients without diabetes.
Revascularization remains imperative to limb preservation and survival in patients with CLTI and diabetes. Endovascular interventions were once considered prohibitive in these challenging patients given the high burden of infrapopliteal disease. However, recent data demonstrate that early revascularization coupled with close surveillance can be very beneficial regardless of approach to revascularization.9-11,17,23 Adam et al reported that diabetes was independently associated with higher repeat target-extremity revascularization after balloon angioplasty, with similar rates of clinical success relative to bypass surgery.25 Similarly, in a recent meta-analysis of several randomized control trials, it was observed that relative to plain balloon angioplasty, both drug-coated balloons and drug-eluting stents had improvement in arterial patency and reduced the need for recurrent below-knee TLR.27,28 Patients with diabetes remain at major risk for calcific disease, which in turn predisposes to higher rates of restenosis, flow-limiting dissection, or vasospasm with endovascular intervention. As such, atherectomy techniques are becoming increasingly more popular for plaque modification and prepping the vessel wall to maximize luminal gain with subsequent balloon angioplasty and/or stenting.
In this study, OA with the Diamondback 360 or Stealth 360 (Cardiovascular Systems, Inc) was utilized in all patients. These OA systems utilize centrifugal force with bidirectional sanding to eccentrically create a luminal channel. In a non-randomized multicenter study, Safian et al reported up to 90% procedural success rates (<30% residual stenosis) with low rates of adverse events and no major amputations at 6 months after OA in infrapopliteal lesions.23 Similarly, adjunctive OA yielded numerically higher procedural success and freedom from TLR than balloon angioplasty alone in CLTI patients at 1 year.29 Our findings indicated that these outcomes can be extended to patients with diabetes that are also treated with OA. However, we observed a significantly higher rate of distal embolization in the cohort of patients with diabetes (Table 3), although the odds ratio did not indicate a significant difference in risk between groups. Therefore, it may be prudent to adopt embolic protection strategies when intervening on this patient population. Recently, CSI received United States Food and Drug Administration approval for the Wirion embolic protection system, a distal embolic protection filter that can be used during OA procedures.30
Our results should be interpreted within the context of the limitations of the LIBERTY 360 study, which was a non-randomized, large, multicenter, observational study. Device selection and optimal therapy were not standardized, and were based on the operator’s discretion. Accordingly, the study groups in our current subgroup analysis had different comorbidities, and no true control group comprised of matched patients with diabetes and CLTI who only received angioplasty without OA. In addition to small sample sizes, there was a near 60% attrition rate observed in both patients with and without diabetes. As such, our study might be underpowered to demonstrate differences in outcomes of OA in patients with or without diabetes. A randomized study or pair-matched cohorts might allow for better generalization of our findings. Likewise, wound extent and infection status contribute to limb loss as much as degree of ischemia. Therefore, utilization of a classification scheme such as the wound, ischemia, and foot infection (WIFI) scoring system may provide a better correlation with clinical outcomes. In this posthoc analysis, such a categorization remained out of reach.
Conclusion
Diabetes and CLTI were associated with higher rates of renal disease, hypertension, obesity, and unhealed wounds, indicating higher rates of severe peripheral ischemia. However, there was no difference in the combined risks of major amputation or death between patients with and without diabetes, with high rates of limb preservation and low MAE rates in both groups at 3 years. A significantly higher rate of distal arterial embolization was observed with OA in patients with diabetes; however, the odds ratio did not indicate a significant difference in risk between groups. These results highlight the potential importance of distal embolic protection during OA in this population. Future trials should focus on the comparative effectiveness of OA in patients with CLTI and diabetes with variable peripheral arterial calcification, chronic total occlusions, and other complex lesion characteristics.
Acknowledgment. The authors thank Ann Behrens and Brad J. Martinsen, PhD, from Cardiovascular Systems, Inc for critical review of this manuscript.
Affiliations and Disclosures
From the 1Department of Surgery, Section of Vascular Surgery, Washington University School of Medicine, St Louis, Missouri; 2University of North Carolina at Chapel Hill Rex Health Care System, Raleigh, North Carolina; 3Adventist Health and Vascular Institute at Adventist Health, St Helena, California; 4Advanced Cardiac & Vascular Centers for Amputation Prevention, Grand Rapids, Michigan; 5Washington University School of Medicine, Division of Molecular Cell Biology, St Louis, Missouri; 6Washington University, McKelvey School of Engineering, Department of Biomedical Engineering, St Louis, Missouri; and 7Veterans Affairs St Louis Health Care System, St Louis, Missouri.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Zayed discloses speaking honoria from Cardiovascular Systems, Inc. for the 2021 AMP Symposium; Dr Adams, Dr Armstrong, and Dr Mustapha report consulting income from Cardiovascular Systems, Inc. Dr Zayed’s research effort was partially supported by R01HL153262, R01HL150891, and R03EB028415. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript accepted October 20, 2021.
Address for correspondence: Mohamed A. Zayed, MD, PhD, Department of Surgery, Section of Vascular Surgery, Washington University School of Medicine, 660 South Euclid Avenue, Campus Box 8109, St Louis, MO 63110. Email: zayedm@wustl.edu